DSM-5 Narcissistic Personality Disorder Criteria: What It Actually Means
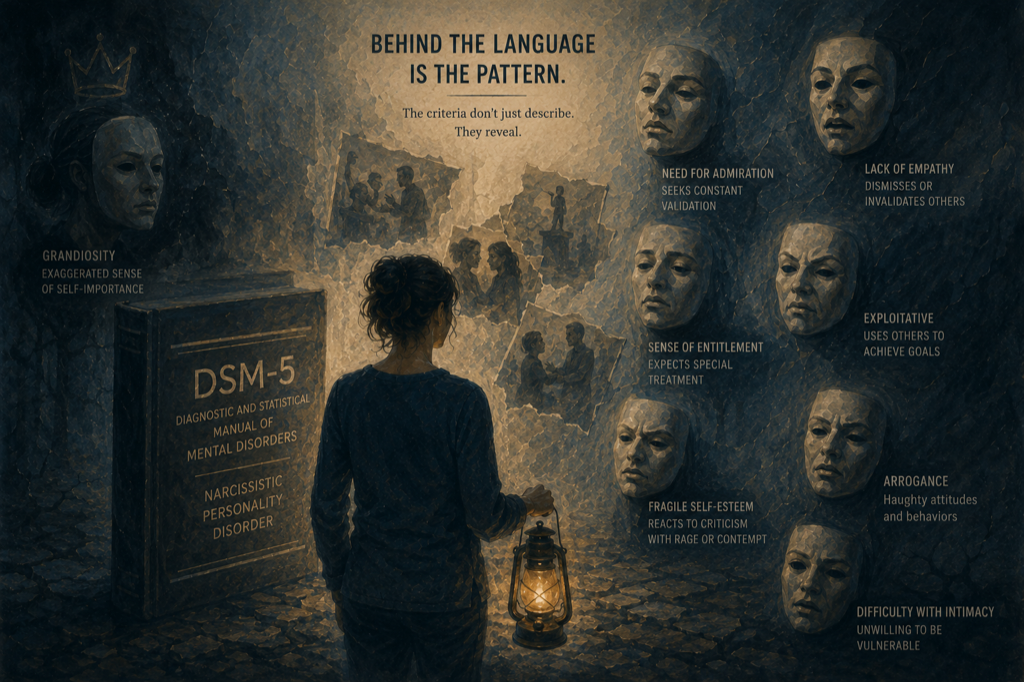
The clinical definition of Narcissistic Personality Disorder lives in the DSM-5 behind language that can obscure what it's actually describing. Translated into plain terms and mapped to real behavior, the criteria become something else: a recognition tool, a framework for patterns that may have felt inexplicable for years.
This isn't a guide for diagnosing anyone. Diagnosis requires a licensed clinician, and a diagnosis changes little about how you protect yourself. What the criteria offer is language and clarity.
The Diagnostic Criteria
The DSM-5 defines NPD as a pervasive pattern of grandiosity, need for admiration, and lack of empathy, beginning by early adulthood, present in a variety of contexts, and indicated by five or more of the following nine criteria.
1. Grandiose sense of self-importance
Exaggerates achievements and talents, expects to be recognized as superior without commensurate achievements.
In plain terms: they believe they are exceptional in ways the evidence doesn't support, and they expect others to treat them as exceptional regardless. This isn't ordinary confidence. It's a fixed belief in superiority that holds even when contradicted by facts.
In relationships: dismissing your concerns as trivial, treating your accomplishments as less significant than theirs, expecting deference as a matter of course.
2. Preoccupied with fantasies of unlimited success, power, brilliance, beauty, or ideal love
The inner life is organized around grandiose fantasies: what they will achieve, who they will become, the perfect relationship they deserve, the recognition that's coming. These fantasies function as regulation: when reality falls short, the problem is always external (others failing to recognize them, circumstances conspiring against them, you not being what they needed).
3. Believes they are special and unique and can only be understood by, or should associate with, other high-status people or institutions
Not everyone is worth their time. They belong with the best: the most successful, prestigious, impressive. This criterion produces name-dropping, status-consciousness, and treatment of ordinary people (including sometimes you) as beneath them. It also produces idealization of high-status people until those people show ordinary-human flaws, at which point idealization can collapse.
4. Requires excessive admiration
This is the supply-seeking behavior many people recognize. The constant need for validation, praise, and positive attention. Conversations that return to them. Fishing for compliments. Irritability or withdrawal when admiration isn't forthcoming. The relationship can feel like a one-way flow: your attention and validation toward them, rarely reciprocated.
5. Has a sense of entitlement
Unreasonable expectations of especially favorable treatment or automatic compliance with their expectations. Rules apply to other people. Their time is more valuable. Their needs take priority. When those expectations aren't met (when you have needs, set a limit, or circumstances don't bend to their preference), the response is often disproportionate anger or contempt.
6. Interpersonally exploitative
Takes advantage of others to achieve their own ends. This doesn't require malicious intent. In many cases other people's needs simply don't register as real constraints on their behavior. You are useful to them, and when you're no longer useful, the relationship changes.
7. Lacks empathy
Is unwilling to recognize or identify with the feelings and needs of others.
This criterion is foundational. It's what makes much of the other behavior possible. If your pain doesn't land, if your needs don't register, there's little restraining the behavior.
Note the DSM language: unwilling. Some clinicians discuss whether capacity for empathy is impaired in some presentations; the DSM-5 criterion text itself emphasizes unwillingness. The functional result for the person on the receiving end is often the same.
8. Is often envious of others or believes others are envious of them
Envy, experienced or projected. When others have or achieve things the narcissistic person wants, it can register as threat or injustice. The projection version: attributing envy to others as an explanation for criticism or challenges. "They're just jealous" as a response to legitimate feedback.
9. Shows arrogant, haughty behaviors or attitudes
Contempt for people they consider inferior. A particular quality of dismissiveness. The eye roll, the condescending tone, the ostentatious boredom with ordinary things. In relationships, this often shows up in devaluation: the shift from idealization to contempt that characterizes the narcissistic cycle.
What the Criteria Don't Capture
The DSM describes a personality disorder in clinical terms. Several things survivors most need to understand aren't in the criteria.
The tactics. Gaslighting, DARVO, love bombing, triangulation: these specific behaviors aren't listed in the DSM. The criteria describe underlying personality structure; the tactics are what that structure can produce in close relationships.
The variability. A person who meets five of nine criteria can present very differently from someone who meets all nine. The covert narcissist who leads with victimhood looks nothing like the grandiose narcissist who leads with superiority, yet both can meet the clinical threshold.
The impact on others. The DSM is organized around the experience of the person with the disorder, not the people in relationship with them. The damage to partners, children, family members, and colleagues isn't in the criteria.
Why Diagnosis Isn't the Goal
People in relationships with narcissistically organized people often spend significant energy trying to determine whether the person qualifies for an NPD diagnosis. That's understandable. A diagnosis would validate the experience, provide a framework, and perhaps convince others.
But the diagnostic question is less useful than it might seem. Only a clinician with sustained access to the individual can diagnose. People cause significant harm without meeting the full clinical threshold for a personality disorder. The harm you experienced is real whether or not the person technically qualifies.
What the criteria offer is recognition. Not of a diagnosis, but of a pattern. Pattern recognition is often exactly what survivors are missing when they can't understand what's been happening to them.
If you're comparing someone's behavior to these criteria using real messages, paste a thread into DARVO.app/analyze. It flags manipulation tactics in plain language without replacing clinical assessment.